
I regularly meet with clients who tell me that they are suffering from something like depression, but... they then go on to tell me that it doesn't feel like depression. I had two clients independently tell me some version of this just yesterday. These clients typically have some combination of problems with their sleep, problems with their energy levels, problems with emotional regulation, they experience a high degree of irritability, report feelings of being overwhelmed, and struggle with decision making/feelings of paralysis. Is this depression? What exactly is depression?

My hypothesis is that this is not depression. To my mind, there is a much better descriptive label that much more accurately describes what my clients are describing in session: anomie. You will not find anomie in the DSM, sometimes referred to as the bible of mental health disorders. And like the actual bible... we should not take it too literally. We shouldn't take what we find in the DSM as canon, because when we look into the history of nosology—the science of classifying and naming diseases—we find that the chapter on depression extremely interesting.
It might sound surprising to hear, but the thing we now know as depression is only 44 years old. Depression in it's current iteration is a product of the DSM-III, published in 1980. 1980 is the year of the birth of Major Depressive Disorder (MDD). In historian Edward Shorter's amazing 2021 book, The Rise and Fall of the Age of Psychopharmacology, he chronicles the ways in which disparate phenomena were claimed by DSM nosologists under the diagnosis of MDD. Prior to 1980, the diagnosis depression referred to extremely serious illnesses, namely melancholic and catatonic depression. These are disease states that regularly require hospitalization and include symptomatology such as the following,
- Mutism (inability to speak)
- Stupor (a state of reduced consciousness and responsiveness)
- Rigidity (stiffness and immobility)
- Complete incapacity to experience pleasure
- Hopelessness and suicidality
- Vegetative symptoms
- Akasthesia (profound agitation and restlessness)
This sort of symptomatology is extremely serious and requires urgent medical attention. But in 1980, the authors of the DSM made what I can only describe as a massive land grab: they took the diagnosis of depression, which had previously been used to categorize persons with the sorts of extreme symptomatology as above, and added broad and non-specific symptoms, such as: sadness, anxiety, irritability, and difficulty concentrating. This land grab was motivated, Shorter tells us for two specific reasons:
- to prevent the psychoanalysts and psychotherapists from using their own nosological categories that arose out of their clinical experience (what I am, in fact, attempting to do here).
- because you need specific diagnostic criteria if you're going to claim that a medication is effective, and... SSRIs were ready to burst onto the scene.
And this is precisely what happened: the DSM-III land grab was successful. DSM nosology edged out the psychotherapeutic and psychoanalytic clinicians and their experience. And SSRIs became the most profitable medications of their generation.
It turns out that though the authors of the DSM-III to our current DSM-V were successful in their land grab, the results for patients over the past 44 years have been poor. Listen again to Shorter describe the result of four decades of "modern" psychopharmacological treatments for depression:
The Age of Psychopharmacology collapsed in the end because of the scientific inadequacy of the diagnostic classification and the therapeutic inadequacy of the SSRIs, which, as they went off patent early in the new century, seemed little better than placebos in the treatment of real depression.
Edward Shorter, The Rise and Fall of the Age of Psychopharmacology, p. 110
It turns out that globally, we collectively took tens of billions of doses of a class of medications that was not substantially more effective than sugar pills. To my knowledge, we have yet to receive an apology—let alone compensation—from the companies whose early research in the 1970s pointed to the relative ineffectiveness of these medications.
Our comprehensive review of the major strands of research on serotonin shows there is no convincing evidence that depression is associated with, or caused by, lower serotonin concentrations or activity.
...This review suggests that the huge research effort based on the serotonin hypothesis has not produced convincing evidence of a biochemical basis to depression. This is consistent with research on many other biological markers. We suggest it is time to acknowledge that the serotonin theory of depression is not empirically substantiated.
Moncrieff, Cooper, et al, The serotonin theory of depression: a systematic umbrella review of the evidence
Please note: this is not a reason to stop taking your SSRIs. Though these medications have a poor record of efficacy, they are not free of side-effects, and this is particularly true when ceasing treatment. For most psychiatric medications, it is important to work with your doctor to taper doses downward.
So... if some of the phenomena we have associated with depression since 1980 are not well named and described! or categorized! or treated! under the diagnostic title depression, what then should we call and how ought we to treat people who struggle in these ways? My proposal is to employ an old sociological term as a descriptor, anomie.
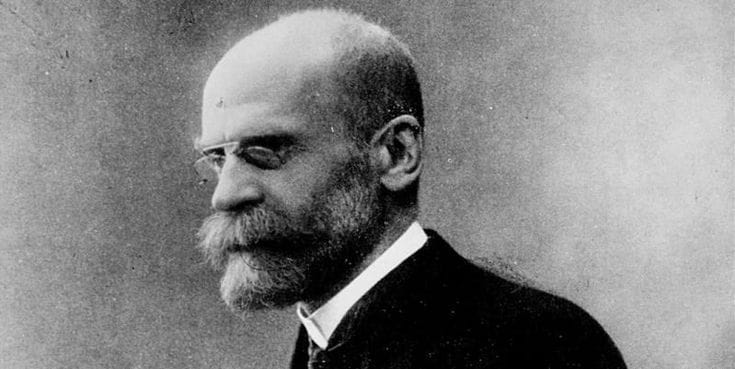
Anomie is a term coined by the French Sociologist, Emile Durkheim, and is most prominently associated with his work on the social causes of suicide. Anomie is not a technically diagnostic term and is not present in any iteration of the DSM. Durkheim's work on anomie dates from the late 19th century, and it was developed primarily a way that he could describe the social forces that contributed to rates of suicide in that era.
Anomie is often associated with another French term, ennui, and depression itself. But anomie has a very distinct definition that separates it from these other terms. Anomie is from the Greek anomia, which means "lawlessness." Anomie refers to the state of a community—remember Durkheim is a sociologist and isn't interested in individuals—that is flux or transition. And in that flux, community members are unsure about the rules that govern daily life. This is what it means to experience lawlessness: to experience a domain specific or global sense of insecurity about how to live one's life.
Let's be more specific: the 19th century was a time of great social upheaval. For instance, the role of women was changing: how should husbands then relate to their wives? How should women think about themselves and their families? For centuries, the roles of men and women were relatively stable. The result was that it was stifling for both men and women, and there were no real fundamental decisions to make about how men and women related.
The 19th century also saw massive migrations, both across borders and from rural to urban. The pace and cycles of life that had been stable for centuries were drastically upended. Those rural folk who moved to urban centres had to find whole new ways to live—and cities of the 19th century were grim affairs for those with lesser resources. This is the meaning of anomie: the inability to rely on the ways you have traditionally understood your purpose, your family and community members, your way of making a living, and, indeed, the very way you understand yourself. There is a modern aphorism that describes this state of things: in the early days of Facebook, the motto was "move fast and break things." This is a good description of what Durkheim found in late 19th century France, and it is a good description of what clients bring into my office on a daily basis. It's just that... the "things" that Zuckerberg and his crew so cavalierly were happy to break were the bonds that held families and communities together for centuries and, indeed, people themselves.
The migrations of the 19th century produced the lawlessness or normlessness that Durkheim found in his studies. The inability to feel secure in one's life means that predicting the future becomes a much more energy intensive undertaking. If you were a farmer in the 18th century, and your family had lived on and farmed that land for generations, the energy you would need to predict and understand your future was minimal. Of course, this meant that there was much less mobility in people's lives—social mobility, class mobility, geographical mobility, etc. But it didn't take a lot resources to know—to really know and trust—how things would work out: like your ancestors, you would farm the land, you would have a family, and if you lived a good and just life, you would go to heaven. That was the future.
Unlike the 18th century farmer whose life was determined by traditional attitudes and community bonds, Durkheim found a profound sense of unease and anxiety and lack of clarity in his late-19th century studies. And this is what I find in my clinical work as well.
Let me add some descriptive language from Durkheim himself and Søren Kierkegaard, who both speak to this problem of lawlessness. Though a sociologist and not a psychologist, Durkheim offers a kind of diagnosis to the social upheaval he sees beyond the language of anomie: he coined the phrase mal d'infini or the sickness of infinitude. A sickness of infinitude comes to pass precisely when the rules, laws, and conventions of a society are weakest, because in the absence of rules, laws, and conventions, anything feels possible. And, if everything is possible, then the work one must do to determine how to live on a day-to-day basis becomes exponentially more challenging. If everything is possible... how to know what to do, how to proceed? This is what Jean-Paul Sartre meant when he referred to the "dizziness of freedom:" one's head spins with vertigo when faced with ungoverned possibilities.
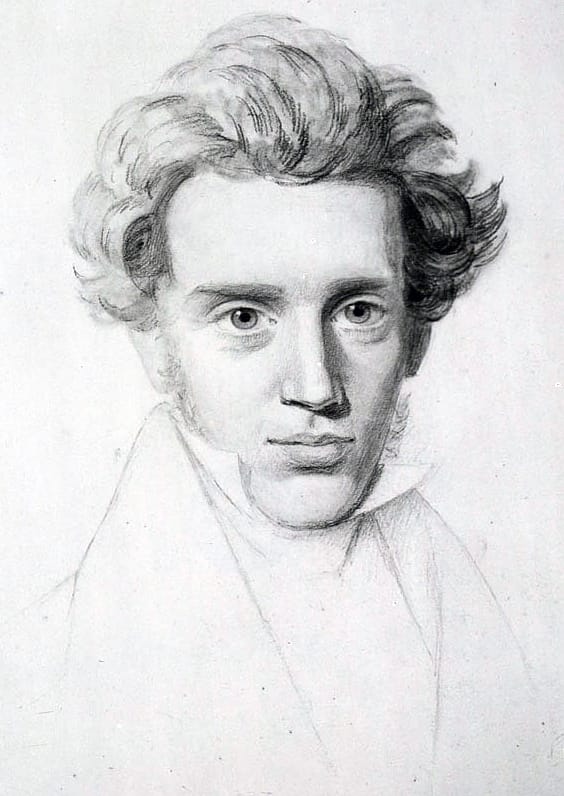
And Kierkegaard, who lived half a century prior to Durkheim in Denmark had eerily similar things to say about the problems of lawlessness. Kierkegaard refers to the phenomena that Durkheim calls mal d'infini as Infinitude's Despair. For Kierkegaard, despair has a variety of causes, but the first one he discusses is a variety that is produced by being subjected to an experience of everythingness. In the following quotation, Kierkegaard refers to "the fantastic," which speaks to the possibilities of one's imagination when the requisite structures do not exist in one's community or oneself.
The fantastic is generally that which leads a person out into the infinite in such a way that it only leads him away from himself and thereby prevents him from coming back to himself.
Søren Kierkegaard, The Sickness Unto Death, Section 144
He goes on to claim that, "When feeling becomes fantastic in this way, the self becomes only more and more volatilized...". I take "volatilized" to mean here dysregulated. And what this suggests is that when there are not sufficient rules and laws and conventions, one's imagination is completely ungoverned. And an ungoverned—"fantastic" in Kierkegaard's words—mind ultimately leads one away from oneself... towards the sickness unto death that is despair.
One last note from the pen of Kierkegaard: he poses a solution. This is what he counsels as the most important intervention a person can make on their own behalf:
Here at once is the principle of limitation, the sole saving principle in the world. The more a person limits himself, the more resourceful he becomes.
Søren Kierkegaard, Either/Or, Section 264
This might strike the reader's ear as odd. Søren Kierkegaard the first—and greatest—of all the existentialist thinkers suggests here not only is it good to create constraints—unfreedoms—for oneself, but that it is "the sole saving principal in the world." Kierkegaard could have said that the "sole saving principal" is freedom or faith or relationship to god or courage or love of self. He doesn't point to the expanse of possibilities but rather says that the sole way forward is through limitation.
Kierkegaard is not only the first of the existentialists but the first psychologist—and he might be the greatest of these too. He gave us all the clues and language to have been able to build a psychology that understood the problem of too muchness, of everythingness, of infinitude. But instead, we ended up with its opposite: a theory of psychology that was premised not on the problem of infinitude and the despair or anomie that follows—but on repression.

